In this post Andrew Petrosoniak discussed the use of tranexamic acid in the prehospital trauma setting, and Auckland HEMS is currently developing a prehospital protocol its use in our service.
About a year ago, Scott Weingart from emcrit.org interviewed Dr Tim Coats, one of the lead authors of the CRASH 2 trial. The interview, which covers a lot of practical territory, became a podcast on emcrit.org in early 2012.
There have been significant changes in the delivery of acute trauma care as a result of the military conflicts in Iraq and Afghanistan. One of the recent advances has been the advent of haemostatic dressings for haemorrhage control, which are now being used in the civilian as well as the military setting.
Auckland HEMS carries a product called Quikclot Gauze. This is an inert mixture of oxides of silica, sodium, magnesium, aluminium, and quartz. The compounds absorb water in a physical (not chemical) reaction, which concentrates platelets and clotting factors at the site of administration.
In 2008 the Journal of Trauma published a case series of the first 103 documented uses of Quikclot, including uses in military and civilian prehospital and hospital settings. The majority of uses involved extremity haemorrhage, often when direct pressure and tourniquets and direct pressure had failed. First responders found Quikclot to be 100% effective. Quikclot was ineffective in a handful of hospital cases, which involved moribund coagulopathic massively-injured patients. Heat generation from the physical reaction was an issue, with 3 patients sustaining burns, and a quarter of concious patients reporting ‘moderate to severe’ pain.
Wound from helicopter rotor blade, with Quikclot applied
There is also evidence from an animal model that Quikclot may allow sufficient haemostasis to reduce tourniquet time. This study involved a pig model of extremity haemorrhage and found that after haemostasis of a bleeding extremity had been acheived with a tourniquet and Quikclot, bleeding occurred only 20% of the time after tourniquet release, compared to a 100% failure rate with standard gauze dressings.
A systematic review of literature regarding haemostatic dressings was published in Injury in 2011, and can be found here. Overall data is scant and mostly observational/retrospective, but what is available suggests that haemostatic dressings like Quikclot should be a useful tool for controlling significant haemorrhage in our prehospital setting.
Full text pdfs for this post are here(secure area limited to ADHB staff only – ADHB has online subscription access to these journals through the Philson Library at the University of Auckland School of Medicine)
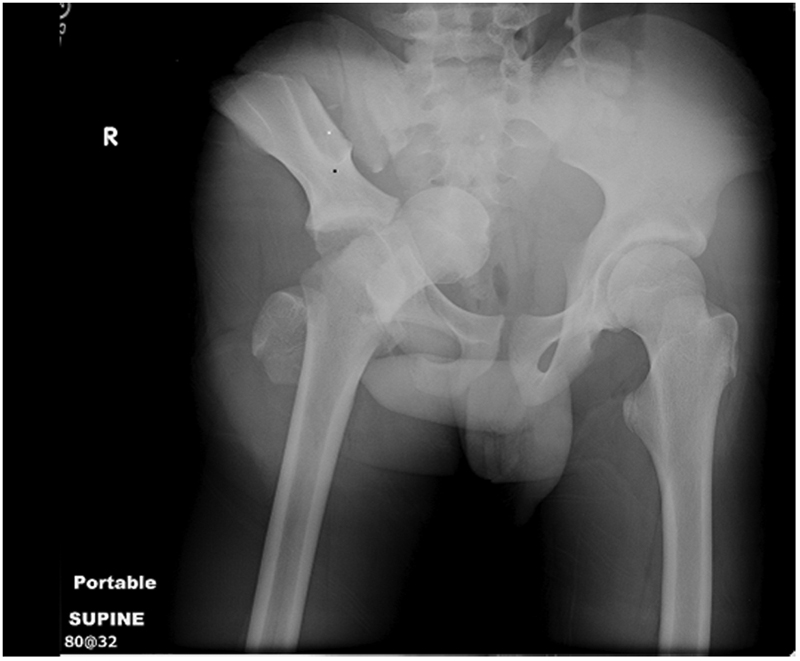
In the New Zealand trauma setting, blunt trauma is by far the most common mechanism. In the Auckland region it is not uncommon for us to manage patients with major pelvic trauma in ED (most commonly as a result of road trauma), and with the advent of the HEMS service our team are now dealing with this in the prehospital setting as well. The most notable case transported by the Auckland HEMS service in the last year involved a middle aged patient with a free-floating pubic symphysis (open bilaterally with actively bleeding groin wounds), a sacral fracture, and an ED arrival blood pressure of 66/40…)
This paper, published in 2007 by a UK trauma service, provides a nice overview of the prehospital management of pelvic trauma.
Take-home messages:
In patients who are obtunded (and therefore have an utterly unreliable clinical assessment) a pelvic fracture should be assumed to be present and a splinting device placed
in conscious patients, the presence of pelvic pain is a more reliable indicator of a fracture than palpation or compression of the pelvis
Reduction and stabilisation of pelvic fractures should occur as soon as possible after injury, while clotting mechanisms are still intact
Bleeding from pelvic fractures should be considered to be non-compressible, and therefore permissive hypotension (resuscitation to the presence of a radial pulse only) should be considered as a resuscitation strategy; NICE guidelines recommend 250mL boluses titrated to the radial pulse
There is a risk of patients becoming haemodynamically unstable following full log-rolls for spinal assessment (this has been reported in the ED setting); in the prehospital setting a roll to 15 degrees only will allow placement of a scoop
the handover to medical staff in ED should include advice not to remove the splint until a significant injury is excluded, including the fact that pelvic splints can provide excellent anatomical reduction leading to fractures potentially being missed and displacing once the splint is removed
The following is an instructional video showing the use of the SAM Sling, which is carried as standard kit on our helicopters: