Scenario involving a rapid ascent resulting in probable CAGE and tension pneumothorax. Medical care including possible RSI and stretcher winch of ventilated patient
Please provide feedback on this scenario below

Scenario involving a rapid ascent resulting in probable CAGE and tension pneumothorax. Medical care including possible RSI and stretcher winch of ventilated patient
Please provide feedback on this scenario below
One of the challenges of resuscitation and pre-hospital medicine is that there are multiple high-risk but rarely performed procedures that clinicians must be ready to perform. The difficulty is that we may go our entire careers and only perform them once or even more likely never. However, the difference from success and failure for these procedures can mean life or limb. Consequently we must remain competent despite the challenges with practice. There is an excellent article that articulates these issues by Cliff Reid & M Clancy which I highly recommend reading (for anyone interested in the topic).
(a primer video I integrated into a recent cric teaching session to get our participants into the mood!)
These life-saving, rarely performed procedures happen to be an interest of mine. It’s a fascinating exercise in education and cognition to maintain competence in performing these procedures yet have virtually no real-life patient practice. The likely result is that clinicians are not competent or they do not remain competent in performing them. More optimistically, some clinicians will maintain their skills through simulation. However, I would bet that a survey of most staff emergency physicians would reveal virtually no hands on practice of many of these life-saving procedures. One of the most talked about and important of these procedures is the surgical airway (or cricothyroidotomy). This is only performed when a patient who requires emergency airway management but they cannot be intubated or ventilated. For most of us, we’ll go through our careers never performing one. But every time we intubate a patient, there’s a risk that this scenario could develop and we’ll have to act accordingly.
At ARHT last week, I ran an inter-professional session for the paramedics, doctors and crewman on surgical airway performance (or cricothyroidotomy). The goal was to integrate our new cricothyroidotomy task trainers into the educational curriculum and combine them with some group discussion and simulation. For those looking to do replicate the event or simply looking for ideas, I will outline our session.
In addition to the introduction of our new task-trainers we also used this opportunity to review our performance of surgical airway. From an educator’s perspective, the most important step for success of this session is preparation. Those who know me, know that I’m not a detail oriented person but planning for everything from big picture stuff to the smallest detail can make a huge difference. In an effort to encourage the sharing of information (FOAMed) I’ll describe our itinerary.
Before the session I sent 2 emails. Our group is relatively new to the flipped classroom, or sending material first then promoting discussion within the classroom/learning site. Something I took home from SMACC 2013 is start with videos (easy to digest material) if you’re implementing a flipped classroom approach for the first time. A follow up email was sent with the videos again and this time along with 2 articles:
Introduction
Content Presentation (using powerpoint)

No better way to encourage participation than some pointing and asking people directly! (not my finest picture during a lecture…)
Task Trainers

Our cric station set up. A variety of equipment that allowed participants to try various methods

Our crew practicing a surgical airway on a task trainer

Several participants trying out a needle jet ventilation techniqu
Brainstorming session
Simulation

Debriefing after the manikin was successfully rescued from under the trailer! He got a cric and was ventilated by our team! Disclaimer…no manikins were harmed during this educational session (except a few cuts to their necks)
Debriefing
This entire process included usability testing for participants – allowing them to use different techniques & equipment they may otherwise not try. This also provides an additional opportunity for inter-professional education that is extremely important for such a high risk, rarely performed procedure. Proper planning and training for all team members involved will only make the process better.
A recent concept that has been widely discussed on FOAM sites, as well as at the SMACC conference, is The Vortex (pdf)
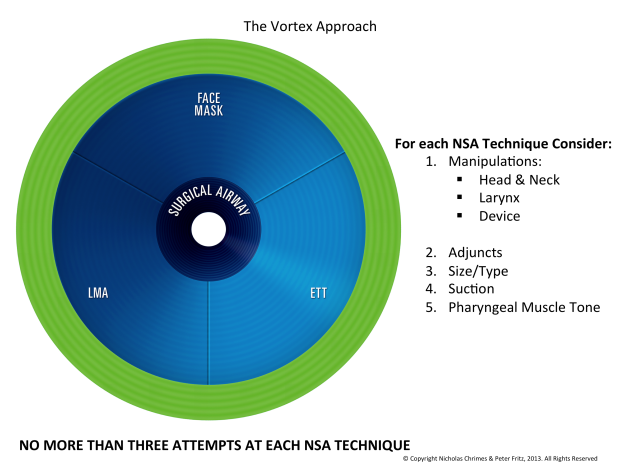
Who needs an algorithm? Here is The Vortex!
The Vortex is a simple cognitive aid that can be used in the setting of an unanticipated difficult airway. Conceived by Nicholas Chrimes (Melbourne anaesthetist) and Peter Fritz (Melbourne emergency physician), it aims to simply concepts, move away from complex algorithims, and be applicable in multiple settings.
Key to the concept is that the key goal in an unexpected difficult airway situation is alveolar oxygen delivery. Techniques to deliver oxygen (LMA, ETT, face mask) are regarded as equivalent, as any of these, if successful, will move a desaturating patient out of the Vortex into the ‘green zone’ where oxygenation is adequate for a ‘time out’ and alternative planning to occur. At the centre of the vortex is a surgical airway.
Resources regarding The Vortex:
Discussion page and podcast from Minh Le Cong, with an interview of the creators of The Vortex
Presentation by Nicholas Chrimes:
The Vortex in action:
Fast-forward to 40 minutes – soldier with severe maxillofacial trauma has scalpel-finger-tube cricothyroidotomy performed under IM ketamine in the back of a Blackhawk
