
By Damjan Gaco, MD, ARHT HEMS Fellow
History
The origin story of checklists goes as follows: A pilot in the 1930’s stepped off a newly built bomber and said something along the lines of “that is too much plane for one person to handle”. In an ever more complicated world, those words echo true today – especially in the field of medicine. For example, the act of intubation carries many steps – all important: pre-treatment, induction, intubation, back-up plans, confirmation of tube placement, post-tube sedation, and post-intubation care. A post written two years ago by then Auckland HEMS Fellow Dr. Robert Gooch outlines this ever-complicated environment, and the ultimate goal of reducing burden on clinicians.

The B17 Checklist – supposedly where it all began
When it comes down to it, checklists were created for two simple reasons – to avoid disaster, or to guide reaction to disaster. During the period after Hurricane Katrina, relief efforts had to be coordinated on scales ranging from the individual to the national level. There were many private companies and local rescue services who rose to the challenge. To quote Atul Gawande in the Checklist Manifesto, ‘They had made the reliable management of complexity a routine’. They took chaos, and made it resemble order. A skilled clinician does this on a daily basis, but problems arise as clinical situations become unfamiliar, or teams become larger – such as an unexpected difficult airway scenario in an Emergency Department resuscitation room.
Usability of a checklist
Usability is, as defined by Merriam-Webster, ‘the ease of use and learnability of a human-made object’. However, even a simple Wikipedia search will show you dozens of pages which would soon convince you that it is a large and complicated field of study. It is the concept of usability that underlies checklist creation, revision, and implementation. Medical checklists that are designed with ease of use and applicability in mind will ultimately be more utilized, with the hope that they will increase patient safety. Dr Gawande states it simply: ‘They are efficient, to the point, and easy to see even in the most difficult situation. They do not try to spell out everything – a checklist cannot fly a plane. Instead, they provide reminders of only the most critical and important steps – the ones that even the highly skilled professionals using them could miss. Good checklists are, above all, practical’.
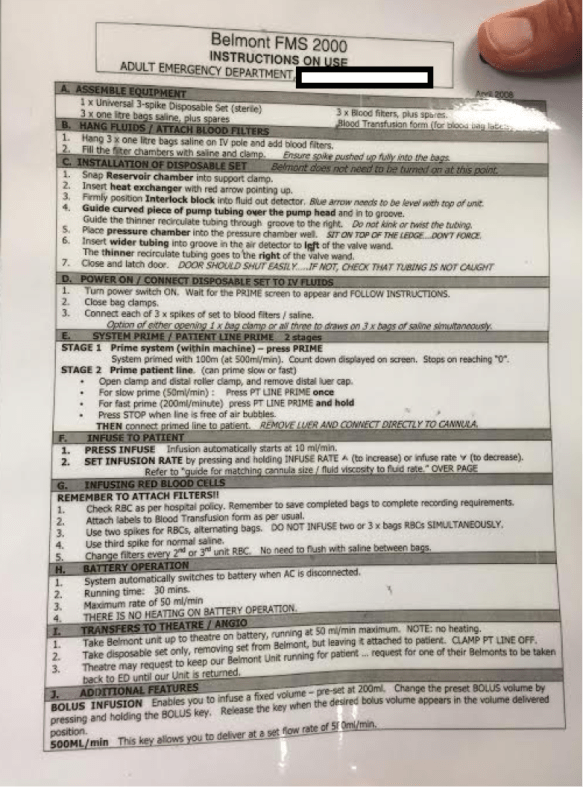
Imagine you were given the checklist above, and told to prime the Belmont Infuser
In 2015, Dr Evans et al. created a Cognitive Aids in Medicine Assessment Tool (CMAT), which was derived from the UK Civil Aviation Authority (CAA) Checklist Assessment Tool. The purpose of this tool was to improve the usability of clinical medicine guidelines. In their own study, they looked at seven published difficult airway guidelines. We thought this was a fantastic initiative – similar to the ‘Checklist for checklists’ created by Project Check. What we found particularly interesting about the CMAT however is that it had its own scoring system, one that we could apply to our own prehospital checklist.
We decided to use the CMAT on a different style of checklist – one that, based on my Medline/ Ovid and grey literature research, appears to be scarcely used in the pre-hospital setting – a post RSI checklist. Post RSI checklists are prevalent in intensive care environments, and to a lesser extent the ED. Websites, such as emcrit.org, have created versions for hospital. In the resource-limited pre-hospital environment, small steps such as remembering to disconnect nasal prongs can have large implications on O2 reserves and transport capacity – thus the need for a post RSI checklist.
A multidisciplinary team of seven people used the CMAT to tailor our post RSI checklist into a version that better adheres to the criteria of the tool. In the month of January, we are performing a survey to compare the two checklists – both criteria-based, and on how usable they appear to be. This survey has a multidisciplinary component: it is offered to crewmen, pilots, paramedics, and physicians. We are optimistic that our new checklist will rate as being more usable, and meeting more criteria that have been established by the CMAT for what constitutes a usable medical tool. We hope that this translates into it being easier to implement and more frequently utilized.

Five of the seven ARHT members, working on the revised checklist
Implementation
So, now that we have a usable product, how do we go about getting staff to buy into our checklists? Stay tuned for the second part of our checklist blog series- as we discuss implementation strategies, and some of the local stories of triumphs.
Damjan Gaco, MD
ARHT HEMS Fellow
Acknowledgements
NASA
Dr Gawande & The Checklist Manifesto
Dr Evans, et al. – the CMAT project
