Medical emergencies present a significant cognitive challenge to the clinician. Multiple causes must be considered and rapidly managed; the consequences of missing a step can be catastrophic. Emergencies in the prehospital setting present the clinician not only with limited time, but also limited space, equipment, and communication.
Aviators have made use of checklists for years to minimize the impact of cognitive errors. Physicians have historically spurned checklists, usually citing their ability to remember an extensive and esoteric differential for just about any physiologic abnormality. Most steps in crisis management, however, are simple enough to be easy to forget under pressure: it doesn’t matter if a clinician can calculate the patient’s shunt fraction if they’ve forgotten to check if the oxygen is connected.
Checklists have made their way into a few areas in medicine already. Pre-op checklists have already significantly improved outcomes at minimal cost.1 Many centres use a checklist for RSI, and operating theatre emergency checklists appear beneficial in simulation trials.2,3 UK HEMS have produced a series of crash cards for emergency situations, but overall the use of emergency checklists in the prehospital setting seems quite limited.
We have produced a series of ‘challenge-response’ emergency checklists. After an emergency is declared, a crew member will read each management step (the challenge) to the clinician, and the clinician will confirm its completion (the response).
Our aim is not to replace a clinician’s judgement, but to reduce the likelihood a management step is missed, and, more importantly, to reduce a clinician’s cognitive burden so challenging steps can be more efficiently completed.
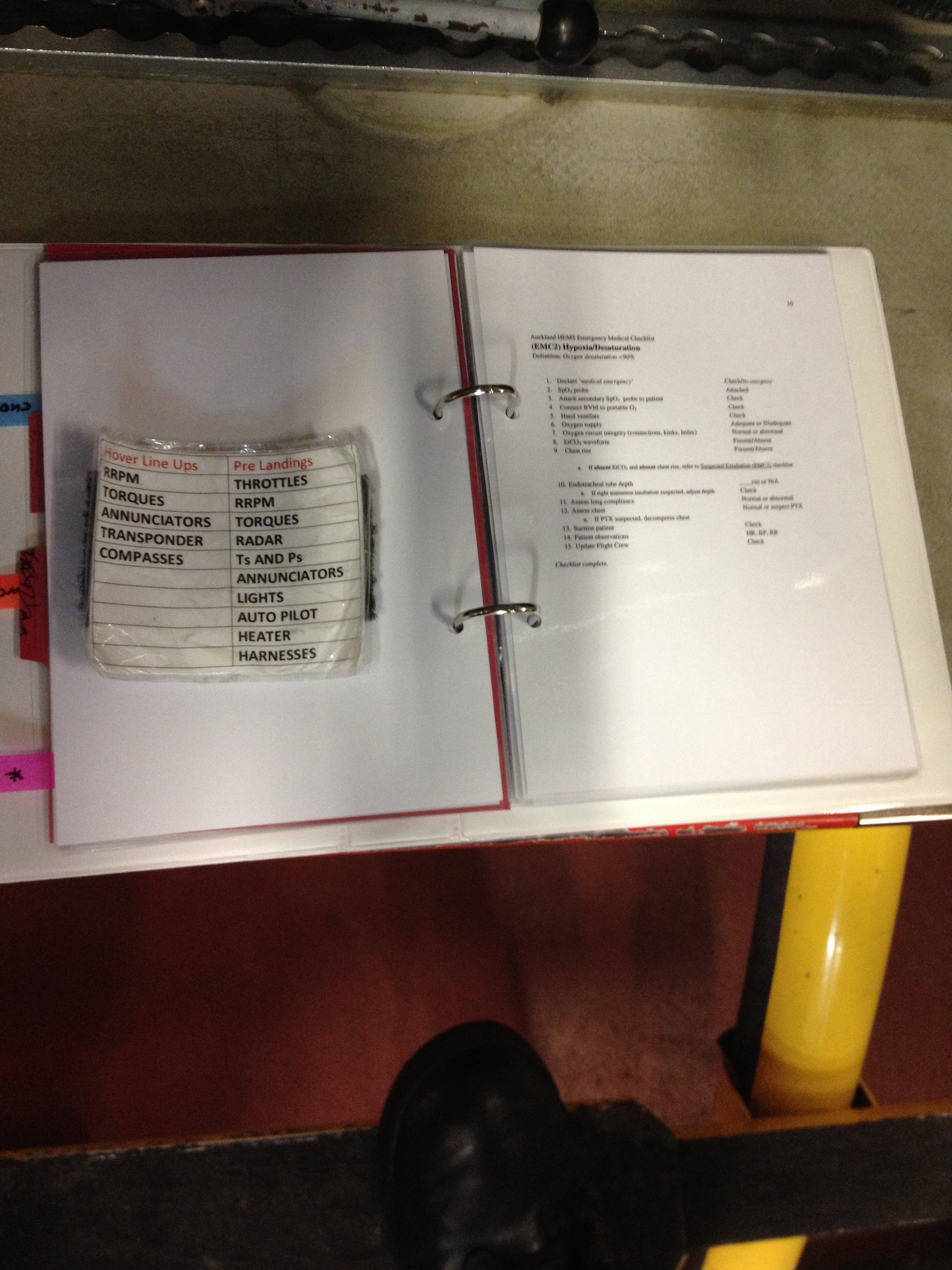
Attached below is our Hypoxia emergency checklist. We’re up to 15 emergency checklists and 4 checklists for standard procedures. We’ve trialled them extensively in a simulated setting at the base, and they’re headed for operational use soon. They’re going to appear in a hard copy format in the helicopter, as well as on the brand new Auckland HEMS app.
Hypoxia Checklist
The preliminary hard copy format:

In-situ checklist testing:

We’d love to hear comments and suggestions – we’re looking to improve these on an ongoing basis. Post any thoughts below or email me directly at rgooch44@gmail.com
References:
1. Haynes AB. Weiser TG. Berry WR. Lipsitz SR. Breizat AS. Dellinger EP. Herbosa T. Joseph S. Kibatala PL. Lapitan MCM. Merry AF. Moorthy K. Reznick RK. Taylor B. Gawande AA. A Surgical Safety Checklist to Reduce Morbidity and Mortality in a Global Population. New England Journal of Medicine. 2009 Jan 29; 360(5):491-9.
2. Arriaga AF, Bader AM, Wong JM, Lipsitz SR, Berry WR, Ziewacz JE, Hepner DL, Boorman DJ, Pozner CN, Smink DS, Gawande AA. Simulation-Based Trial of Surgical-Crisis Checklists New England Journal Of Medicine 2013;368:246-53.
3. Ziewacz JE, Arriaga AF, Bader AM, Berry WR, Edmondson L, Wong JM, Lipsitz SR, Hepner DL, Peyre S, Nelson S, Boorman DJ, Smink DS, Ashley SW, Gawande AA. Crisis Checklists for the Operating Room: Development and Pilot Testing Journal of the American College of Surgeons. Aug 2011; 213(2): 212-217.