Several months ago, our HEMS service introduced a portable ultrasound machine onto our helicopters and so far it has been a great success! While this blog post won’t be presenting the data we’re collecting, our physicians have reported it to be extremely useful. Most often we use it in the evaluation of a trauma patient to perform an eFAST (extended focused assessment with sonography in trauma) that includes assessment for free fluid in the abdomen but also importantly, lung ultrasound for the diagnosis of pneumothorax. Recently, I was part of a mission to transport a patient who had suffered a fall and there was question of a pneumothorax as reported by the ambulance team on scene. We were quickly able to perform an ultrasound of the lungs which ruled out pneumothorax. This enabled our pilot to fly at normal altitude rather than having to fly lower. Furthermore, as a clinician, it helped with decision making during transport as the patient still required treatment in hospital for other injuries. Knowledge that a pneumothorax was virtually unlikely allowed me to focus on other treatment priorities.
We’re using a similar model of portable ultrasound as pictured above at ARHT
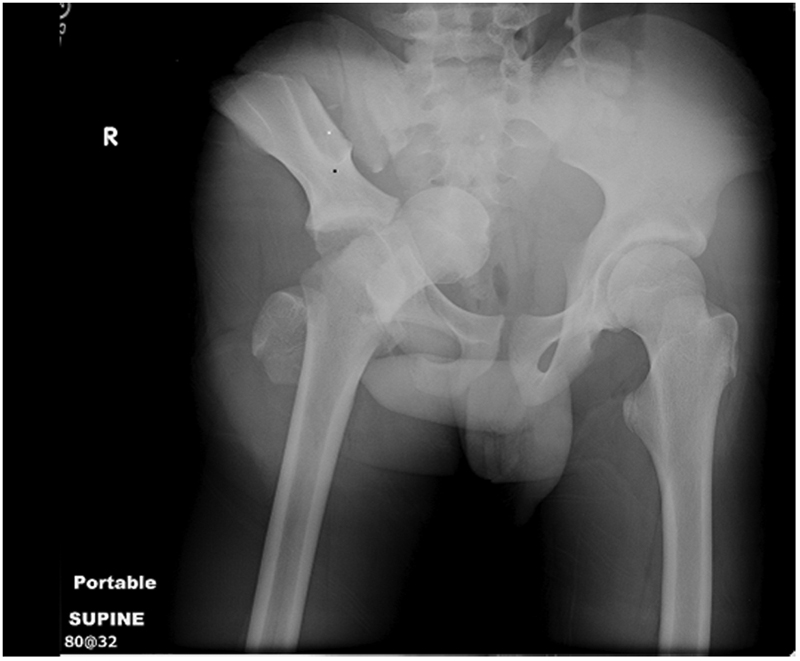
More recently, one of our physicians performed an ultrasound guided femoral nerve block to assist with pain management of a patient with a femur fracture. It worked brilliantly and the patient was transported with considerably less pain!
In the spirit of our new technology, I’ve reviewed what’s out there in the literature regarding prehospital ultrasound (and emphasis on HEMS). There’s very little but this is definitely a growing field!
A recent review of HEMS pre-hospital ultrasound feasibility was published with good results. They performed 144 pre-hospital scans. On average scans took less than 2 minutes with a symptom based approach to what region to scan. While there are some limitations in their methodology, they reported no false-positives compared with available clinical data which is important. In addition, overall sensitivity was 85% (though it should probably be reported for each indication). Nonetheless, this study adds support to the feasibility of prehospital HEMS ultrasound and documents what findings may be value in the field. In several cases, management was altered, for example when pneumothorax was diagnosed then chest drains were placed.
Another study just published, prospectively evaluated the utility of lung ultrasound in non-trauma patients with dyspnea in a pre-hospital setting. They used a focused approach (as pictured below) to specifically identify potential causes of dyspnea. In 68% of cases, physicians reported lung US as a useful tool.

Imaging sites for rapid assessment of lung using ultrasound in dyspneic patients in prehospital setting
They required physicians to complete the exam within 5 minutes as not to delay scene times. Pneumothorax was accurately ruled out in all cases, while a large pericardial effusion causing hemodynamic instability was properly diagnosed though it was only drained once in hospital. You might imagine however that if the patient deteriorated en route that emergent pericardiocentesis would probably be the next intervention so identification would be important.

Algorithm for evaluation of dyspneic patient in the prehospital setting with ultrasound in conjunction with imaging sites of above picture.
I’m not sure how to interpret their results when they reported that additional management approaches were taken in 25% of cases as a result of US. Primarily diuretics were administered after US given the diagnosis of pulmonary edema. In our setting, we don’t carry furosemide so this doesn’t directly apply though if perhaps properly delineating between pulmonary edema and COPD would be useful as nitroglycerin vs. nebulizers could be emphasized in subsequent therapy.
I believe that most of the benefit of prehospital ultrasound is in the injured patient however, as we see, there is growing evidence that it can be used similarly to how it’s used within the emergency department and ICU.
References
1. Eur J Emerg Med. 2010 Oct;17(5):254-9. doi: 10.1097/MEJ.0b013e328336ae9e. Prehospital ultrasound in emergency medicine: incidence, feasibility, indications and diagnoses. Hoyer HX et al.
2. Eur J Emerg Med 2012 Jun;19(3):161-6. doi: 10.1097/MEJ.0b013e328349edcc. Prehospital chest emergency sonography trial in Germany: a prospective study. Neesse A et al.