Auckland ED is conducting a lot of simulation training currently, with a recent focus on airway management.
Last week a teaching session was delivered by Sam Bendall (an Auckland HEMS doctor) on ‘intubation as a team sport’, which covered human factors in ED airway management and included the use of adjuncts like airway checklists. While Auckland HEMS has an RSI checklist, a similar tool has not been finalized for Auckland ED – this is under consideration currently. Following that teaching session, several airway checklists had nonetheless made their way into our resuscitation areas.
High-fidelity simulation training took place this afternoon, led by Sam, Mike Nicholls (another HEMS doctor), and Nancy Mitchell (Nurse Educator).
The first scenario involved a relatively junior team undertaking an emergent RSI. They performed admirably, and the outcome in practice would have been safe and successful. As an observer however, it was apparent that an airway checklist would have contributed to their confidence and comfort levels. (My personal opinion is that we should start using a checklist for ALL ED RSIs, independent of team seniority)
While watching the simulation I spotted a checklist taped to a whiteboard on a side wall. I assumed that was the airway checklist, and thought ‘that’s a clever position – it means the airway assistant can read out the checklist immediately prior to the RSI. They haven’t used it, I must bring this up at the debrief’.
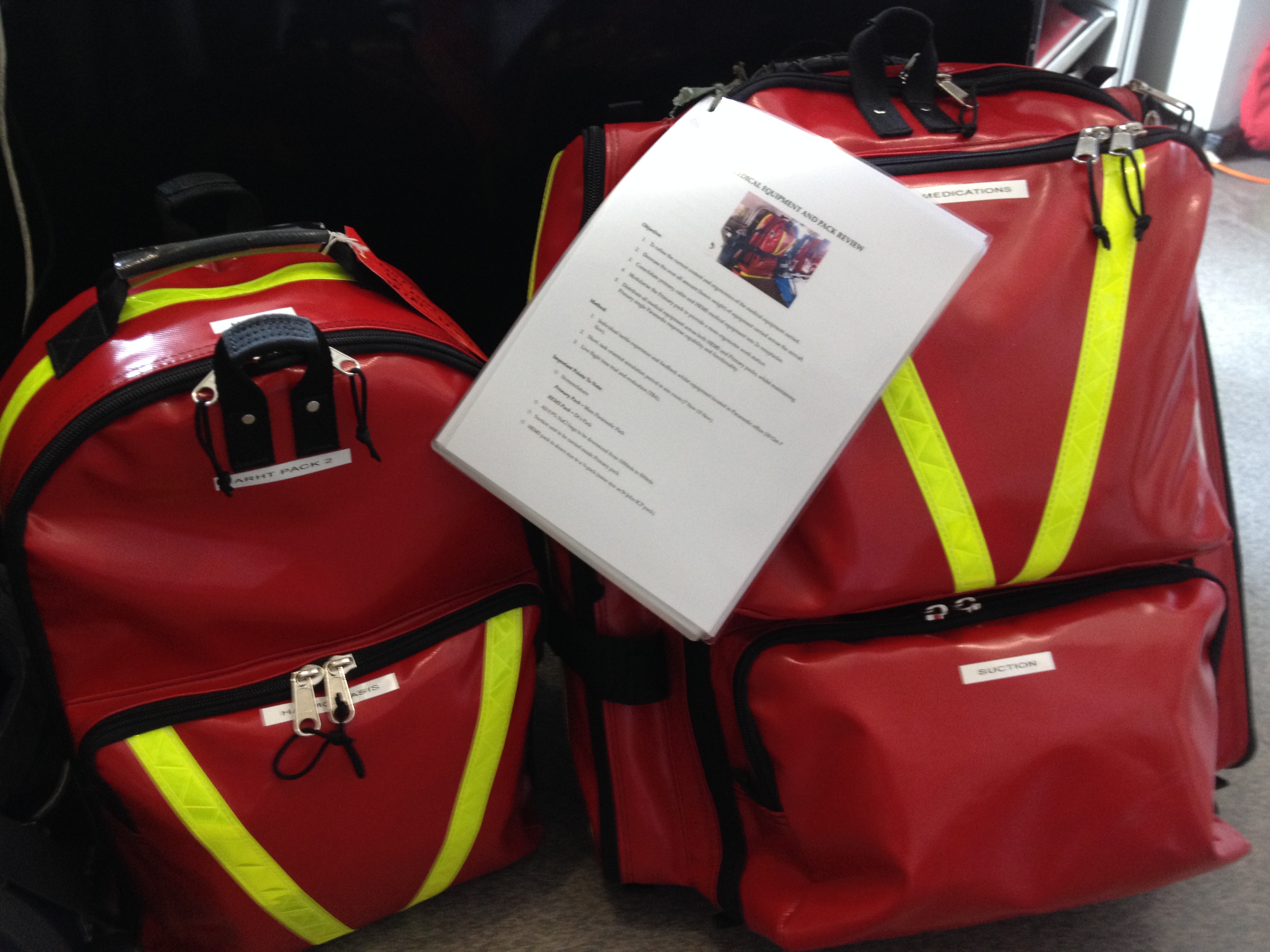
At the end of the debrief, I inspected what I thought was the airway checklist, and found this:

It wasn’t an airway checklist at all, but a restocking checklist!
The actual airway checklist was here…

Tray following RSI (this is NOT how we set up!) Airway checklist bottom left
… taped to the top of the airway trolley (logical) but unfortunately covered up by the airway tray, which is removed from the trolley and placed on top when setting up for airway management. This is a good example of a latent hazard.
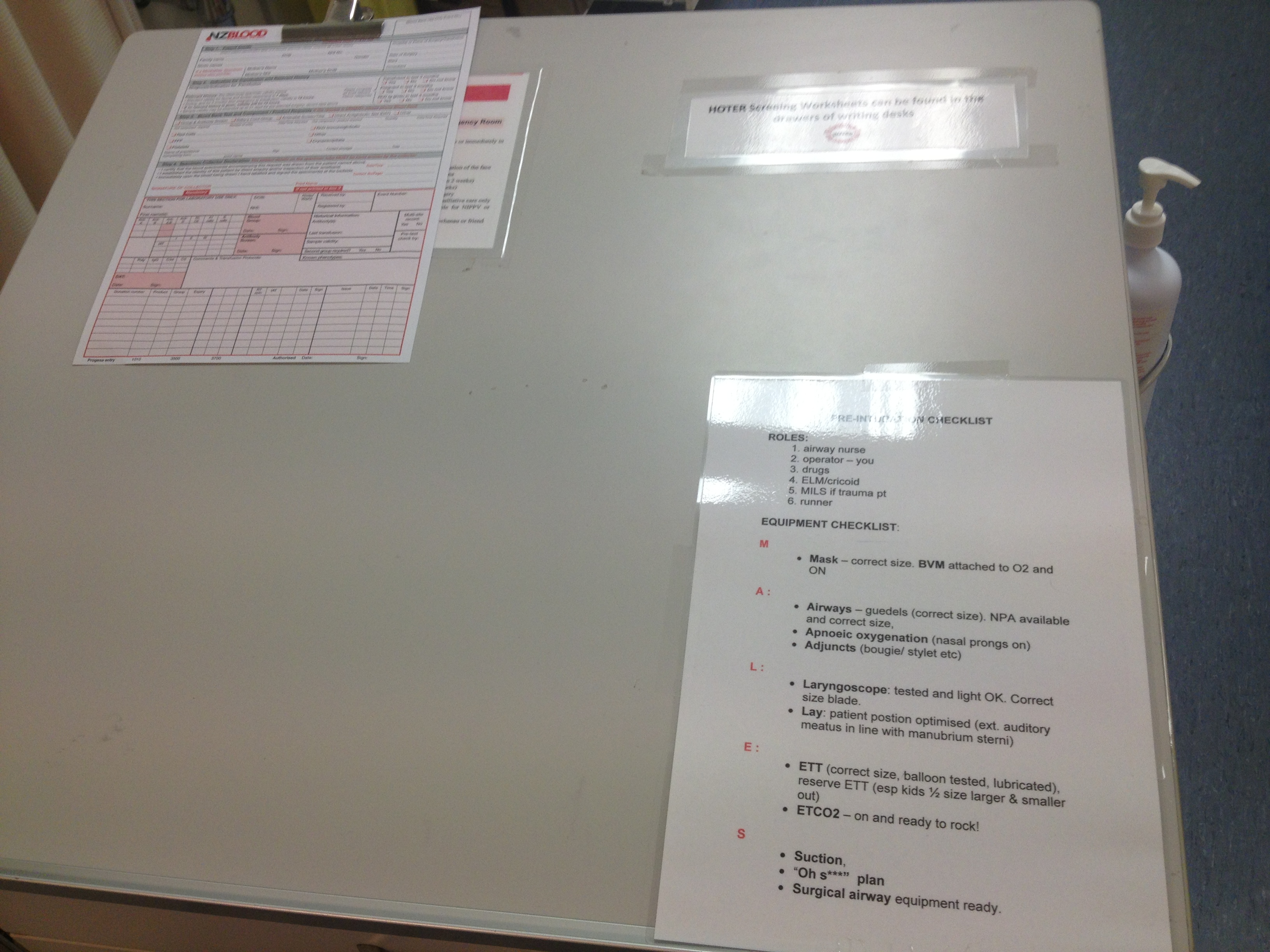
I found a second copy of the checklist taped to the desk at the entrance to the resus bay – this is where the scribe (usually one of the senior nurses) stays during a resuscitation:
 Although this desk is frequently cluttered with paperwork during a resuscitation, accessing the checklist would be a simple matter, and would be done so by a senior person.
Although this desk is frequently cluttered with paperwork during a resuscitation, accessing the checklist would be a simple matter, and would be done so by a senior person.
After looking at the positioning of these checklists, I came to two conclusions:
1) Simulation is a powerful tool for testing the usability of a new item or technique and identifying hazards
When considering logistics/ergonomics/equipment what actually happens in real life may differ from what we envisage mentally when we introduce something new. Simulation introduces stress, time-urgency, ergonomic elements and personnel elements that can rapidly reveal whether something new is going to be useful or not, or whether its introduction has inadvertently created hazards
2) We need to actively manage the environment we work in
When confronted with a critically ill patient, it is easy to focus on the scenario in front of us (there is usually quite enough to think about there!) and accept the physical environment as it is. By going a step further and ACTIVELY managing our environment to improve logistics and ergonomics we can increase our chances of a good outcome. This can occur both BEFORE we are confronted with a patient (eliminating the latent hazard above, for example) and DURING a resuscitation. This is particularly important in the pre-hospital setting, where both the relatively unforgiving helicopter and roadside environment provide a range of challenges not encountered in a resuscitation bay. As doctors I believe we have a lot to learn from our paramedic colleages in this area.
(NB – if someone becomes angry because that restocking checklist mysteriously disappears this week, I had NOTHING to do with it, nothing at all)