
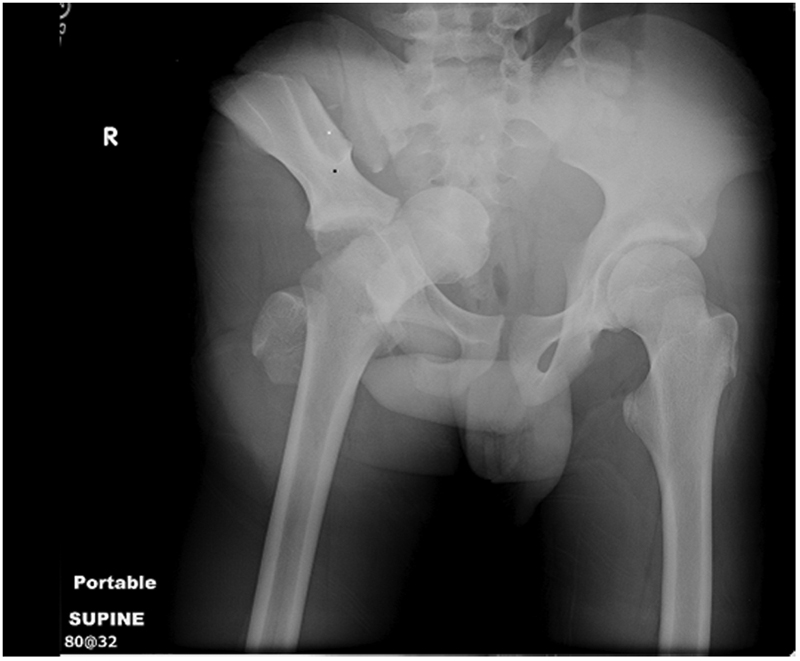
Will a pelvic binder help this?
In the New Zealand trauma setting, blunt trauma is by far the most common mechanism. In the Auckland region it is not uncommon for us to manage patients with major pelvic trauma in ED (most commonly as a result of road trauma), and with the advent of the HEMS service our team are now dealing with this in the prehospital setting as well. The most notable case transported by the Auckland HEMS service in the last year involved a middle aged patient with a free-floating pubic symphysis (open bilaterally with actively bleeding groin wounds), a sacral fracture, and an ED arrival blood pressure of 66/40…)
This paper, published in 2007 by a UK trauma service, provides a nice overview of the prehospital management of pelvic trauma.
Take-home messages:
- In patients who are obtunded (and therefore have an utterly unreliable clinical assessment) a pelvic fracture should be assumed to be present and a splinting device placed
- in conscious patients, the presence of pelvic pain is a more reliable indicator of a fracture than palpation or compression of the pelvis
- Reduction and stabilisation of pelvic fractures should occur as soon as possible after injury, while clotting mechanisms are still intact
- Bleeding from pelvic fractures should be considered to be non-compressible, and therefore permissive hypotension (resuscitation to the presence of a radial pulse only) should be considered as a resuscitation strategy; NICE guidelines recommend 250mL boluses titrated to the radial pulse
- There is a risk of patients becoming haemodynamically unstable following full log-rolls for spinal assessment (this has been reported in the ED setting); in the prehospital setting a roll to 15 degrees only will allow placement of a scoop
- the handover to medical staff in ED should include advice not to remove the splint until a significant injury is excluded, including the fact that pelvic splints can provide excellent anatomical reduction leading to fractures potentially being missed and displacing once the splint is removed
The following is an instructional video showing the use of the SAM Sling, which is carried as standard kit on our helicopters:





