I have just had the pleasure of attending the SMACC (Social Media And Critical Care) conference in Sydney – wow!
Any thoughts that this conference was going to be the same as many college scientific meetings were rapidly dispelled when the (alleged) ‘welcome’ speaker, who was delivering a tedious stuttering analysis of statistical irreleventia was picked up and thrown from the stage (with his lectern) by a masked wrestler wearing the SMACC logo.
Another one bites the dust! Photo from prehospitalmed.com
From the first sessions of the conference it became rapidly apparent that most of the audience were far more Twitter-literate than I was. At first I thought it was a sign of rudeness that over half the audience were tapping away on various mobile devices while speakers were delivering their talks; I then realized that most of the activity was people sending out ‘tweets’.
Each person was tweeting to several hundred people at once.
Tweets contained the speaker’s key ‘take home messages’ and pearls of wisdom, complete with pictures, slides, and links to resources.
It dawned on me that this was instantaneous dissemination of cutting-edge medical information and ideas across oceans and borders.
(plus, of course, the presumably drunken tweet from the Gala Dinner: “F@#$ yeah! This vegan dinner is the s#!t!”)

AucklandHEMS in action: Chris Denny competing in Sonowars
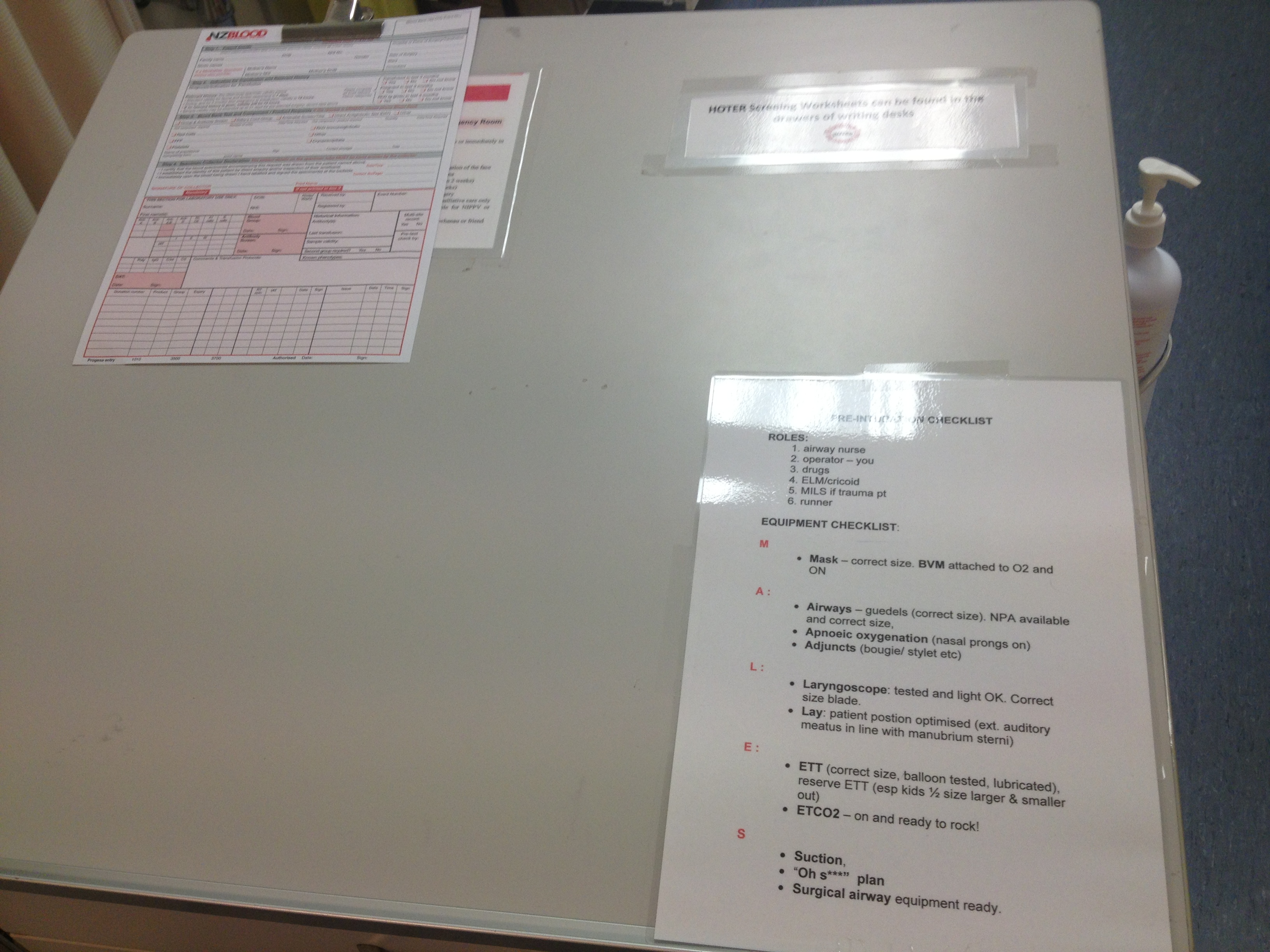
The power of social media for medical use was brought home to me in a talk delivered by Minh Le Cong about airway management.
He played a video of a recent intubation he performed in the retrieval setting., involving a combative patient with a predicted difficult airway, hypoxia despite high flow oxygen via a non-rebreather, and bilateral pneumonia.
This is the sort of clinical scenario that gives acute care doctors and paramedics nightmares, but Minh navigated it successfully with a delayed sequence intubation (premedication with fentanyl allowing enough behavioral control to pre-oxygenate), pre-oxygenation with BiPAP instead of a traditional BVM, providing apneic ventilation with nasal cannulae during the period of paralysis, and placing a Fast-Track (an intubating LMA device) prior to passing a tube through it.
Some of the key elements of airway management listed above have been disseminated largely through social media over the last year. They have been blogged, tweeted, podcasted, vodcasted, and facebooked – not just the techniques themselves but people’s experiences, cautions, and refinements. The end result is that changes in practice have occurred in a timeframe that five years ago would not have been possible. Relying on traditional media (peer-reviewed journals and textbooks) places the timescale for changes in clinical practice into years.
Scott Weingart explains why patients drop their blood pressure once anaesthetised
Clearly there are risks associated with this sort of process. The internet represents pure anarchy when it comes to information dissemination, and it would be very easy for dangerous misinformation to be presented as gospel, aided by slick-looking multimedia pieces (have a look at some of the NZ anti-immunization websites if you want to see misinformation presented in a nice-looking pseudo-scientific form!). A considerable proportion of the conference involved discussions around ways dealing with the uncontrolled nature of FOAM (free open-access meducation) via social media – whether regulation and oversight is needed, how to deal with disputes and misinformation, and how academic colleges (which rely heavily on preset curriculums and traditional media).
The answers to these questions are far from clear.
Having spent the SMACC conference observing the power of social media (specifically for FOAM), I came to the following conclusions:
1) Social media for FOAM is tremendously powerful, and it is here to stay. We should embrace it as a teaching tool.
2) The power of FOAM lies in the ability to transmit not just medical information, but EXPERIENCE – i.e valuable lessons that you would otherwise learn the hard way in resus or on the road.
3) Although there are risks in using FOAM, the benefits vastly outweigh them.
4) There is a moral (but possibly not legal) responsibility on the part of someone producing/disseminating FOAM material to ensure that it is as accurate as possible.
5) The legal responsibility for translating FOAM material into clinical care ultimately lies with the clinician who provides care to the patient
Conclusion 5 is potentially vexatious for clinicians – how do we know what is valid/safe and what is not? Stating “I got this technique from a blog’ is not a defence in the setting of a medicolegal disaster.
The way I have reconciled this is that before applying FOAM material in clinical care, I must make a judgement as to the safety of information, the validity (or otherwise), how and whether it applies to the patient in front of me, how to manage the risk, what the accepted standard of care (and the supporting evidence) is in similar situations, and whether my decision would be defensible in the event of a poor outcome.
Sounds like a complicated and risky process, doesn’t it?
It’s called the Art of Emergency Care, and whether FOAM is involved or not, we are ALREADY doing it every day.