We are delighted to announce the release of the Auckland HEMS mobile app!
————————-
ALERT! January 2015: Since the publication of this post the app has been updated, including the launch of the Auckland HEMS simulation-based prehospital care curriculum podcasts. You can read about the latest additions by clicking HERE
————————-
This app is a work in progress, and will be a living, dynamic project.

Auckland HEMS home screen
We are very keen to have feedback regarding app development and improvement from the prehospital, aeromedical, and emergency medicine communities.
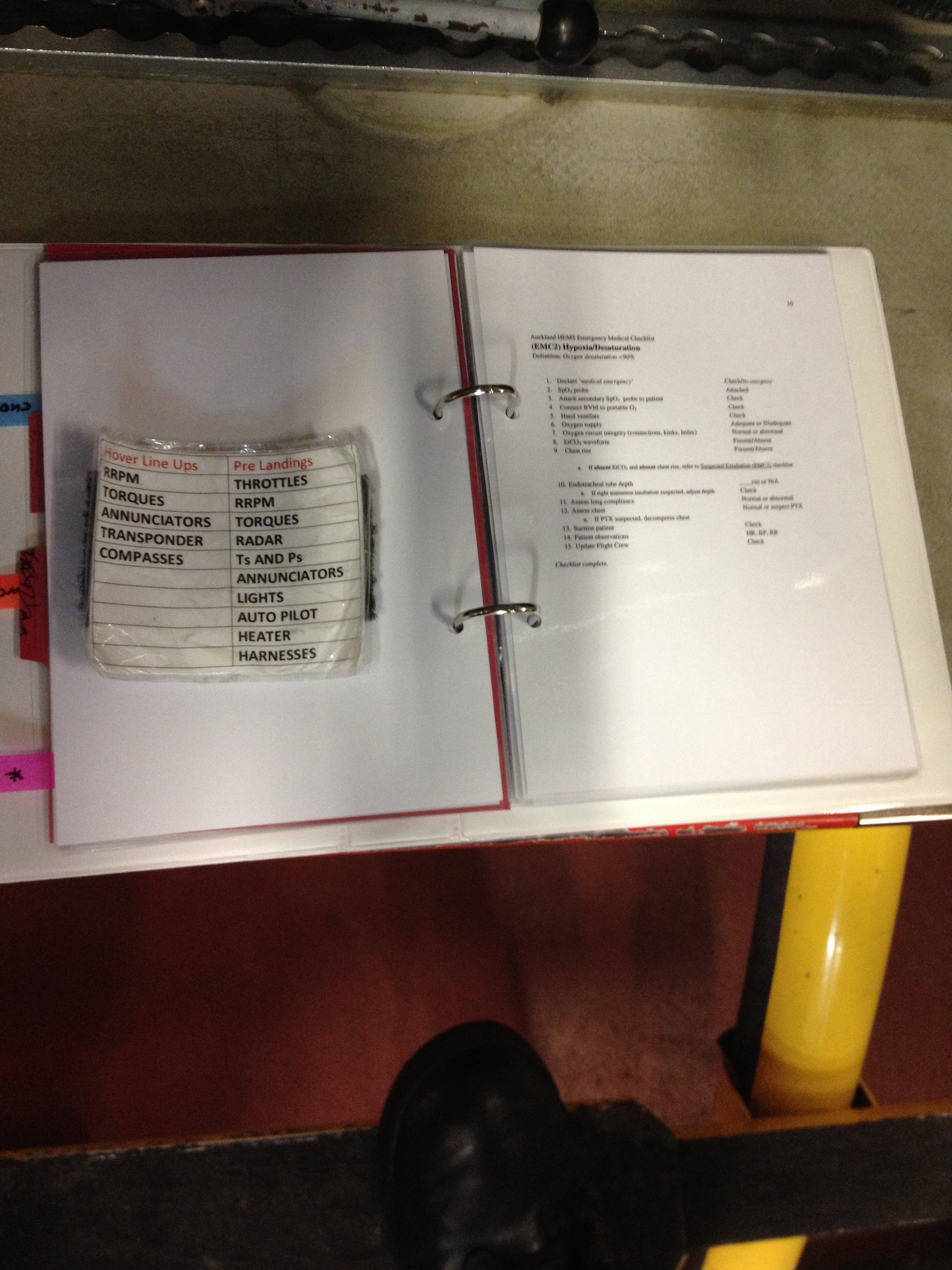
At the heart of the app are the emergency situation checklists that have been developed by Dr Robert Gooch (Canadian Emergency Medicine trainee and recent Auckland HEMS Fellow) and Dr Chris Denny (Auckland HEMS Medical Director).
Auckland HEMS also gratefully acknowledges the efforts of the pilots, paramedics, and crewmen who took place in the simulation-based usability-testing of the checklists, the work of Atul Gawande, and the international HEMS fellowship for allowing Dr Gooch to complete this patient safety initiative.
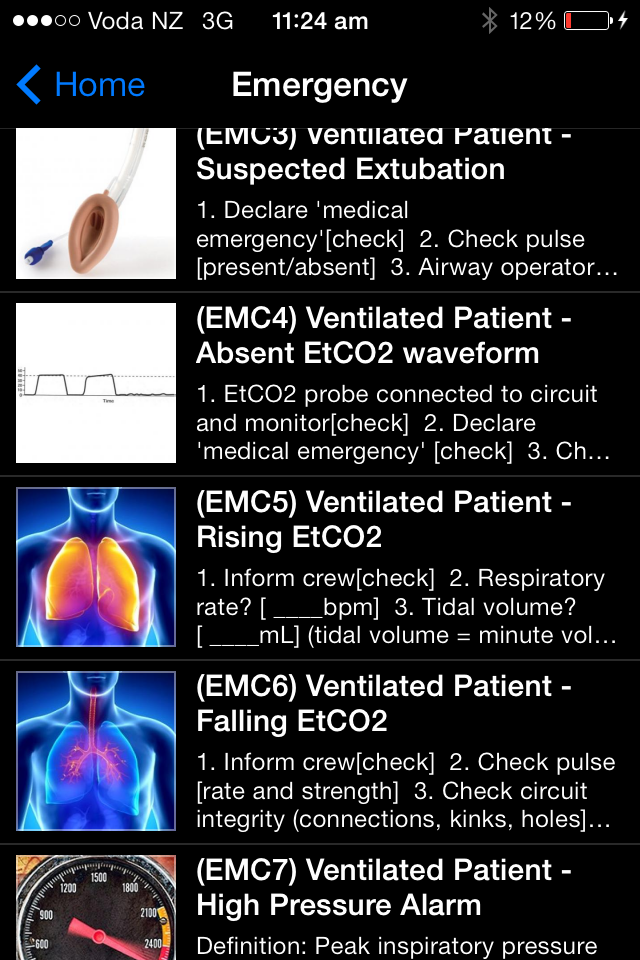
emergency checklist menu
The app also contains other clinical and non-clinical resources.
How can we make it better? We would like to hear your thoughts.
Please use the feedback button in the app, or post comments below.
The app was developed using a platform called ‘ibuildapp‘. This is a web-based subscription service that has the following features:
- straightforward user interface to construct and test the app – if you can create a powerpoint presentation, you can build an app!
- NO coding required
- apps created are functional on both iOS and Android
- immediate updating – alterations to the master version will appear on user’s versions the next time they open the app
- low startup costs compared to having an app professionally coded
The monthly subscription cost to Auckland HEMS increases as more users download the app. As a result we have had to introduce a small charge for iOS users to offset our ongoing costs. Due to some inflexibility regarding price alterations on Google Play (and a failure to read the fine print!), the app will remain free for Android users – it’s your lucky day…
No individual will make a personal profit from this project; any income above our development and subscription costs will go towards further app development and other Auckland HEMS educational and training activities.

Our vision is to use a large team of ‘test pilots’ to make the app as effective as possible for clinical and operational use prior to creating a professionally coded ‘Auckland HEMS 2.0′.
ARE YOU UP FOR THE CHALLENGE?

A test pilot who WAS up for the challenge: Chuck Yeager and the Bell X1
Some improvement suggestions will be possible within the technical features of ‘ibuildapp’, but many will not, and these will be added to the future development list for version 2.0.
TO DOWNLOAD THE APP:
Click HERE for iOS users
Click HERE for Android users
Thank you for being a part of the Auckland HEMS team!